

Ever get one of those texts from a friend asking about the latest miracle supplement? My buddy Marcus sent me a screenshot last month. Some guy at his gym was raving about a “new fat burner” called tesofensine, said he’d ordered it off a website that also sold, no joke, protein powder and t-shirts. Marcus wanted to know if he should get some too.
Here’s the thing. Tesofensine is real, and the data behind it is genuinely interesting. But the question Marcus should have been asking wasn’t “does this work,” it was “who is standing between me and this molecule when I take it.” That second question matters more than people realize, and it’s the one nobody at the gym ever brings up.
Let me be straight with you: tesofensine reaches people through three completely different doors in this country, and only one of them has someone checking your pulse before you walk through. This isn’t sold here, nothing on this page links anywhere you can buy anything, and every claim I make traces back to an actual trial or filing. I just want to walk you through the three doors the way I’d walk Marcus through them if we were sitting at his kitchen table.
The molecule, quickly, because it matters for everything after
Tesofensine (it was originally coded NS2330, in case you see that name floating around) is not a peptide and it’s not a GLP-1 drug like semaglutide or tirzepatide. It’s a small molecule, a triple monoamine reuptake inhibitor, which is a fancy way of saying it keeps serotonin, norepinephrine, and dopamine hanging around longer in your brain. That’s closer cousin territory to some antidepressants and stimulants than to the injectable weight-loss drugs everyone’s been talking about the last few years.
That mechanism is exactly why the “which door” question is so important. It gives tesofensine a specific, well-documented risk profile, cardiovascular and interaction-heavy, and the three doors handle that risk in wildly different ways.
Before I rank them, three facts need to sit with you, because they’re the yardstick everything else gets measured against.
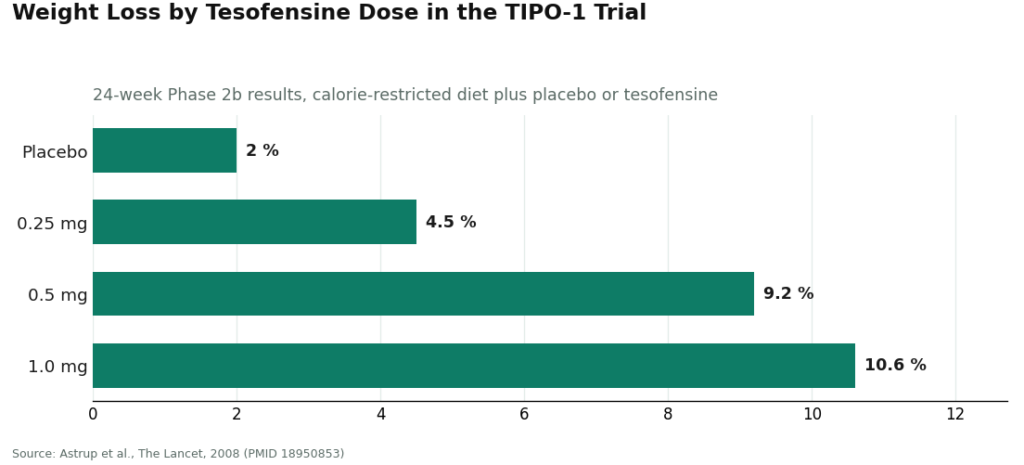
The upside is real. In TIPO-1, a Phase 2b randomized, double-blind, placebo-controlled trial, 203 people with obesity on a calorie-restricted diet lost an average of 4.5%, 9.2%, and 10.6% of body weight at 0.25, 0.5, and 1.0 mg doses over 24 weeks, against 2.0% for placebo [P1]. That’s a meaningful result. The trial’s own authors said it “needs confirmation in phase III trials,” and 17 years later, in the US, that confirmation still hasn’t produced an approval [P1].
The cost shows up in your heart rate. At 0.5 mg in TIPO-1, heart rate climbed about 7.4 bpm. The top 1.0 mg dose got dropped partly over blood pressure concerns, and a separate 2008 meta-analysis found the same heart-rate bump even in patients who weren’t dieting, which confirms it’s the drug doing it, not the calorie cut [P1][P2]. The people developing the drug were worried enough to run a study pairing it with a beta-blocker to cancel out the effect. That study itself got halted over safety concerns [P5].
And the interaction list is a minefield. Because it blocks serotonin reuptake, tesofensine clashes dangerously with MAOIs, SSRIs, SNRIs, stimulants, and bupropion, drugs that a huge number of Americans are already taking for depression, anxiety, or ADHD.
Keep those three facts in your back pocket. Now let’s walk through the doors.
Door one: the FDA-approved version
This is the shortest section I’ll write, because this door doesn’t exist. Tesofensine has no FDA approval, not for weight loss, not for anything. It’s classified as an investigational drug in the US. The furthest it’s gotten anywhere in the world is a favorable technical-committee opinion from Mexico’s regulator, COFEPRIS, in early 2023, which is a procedural nod, not a green light, and not something the FDA had any part in. The rights passed from NeuroSearch to Saniona back in 2014, and the late-stage work since then has run through a partner called Medix in Mexico, outside any FDA pathway. As of 2026, there’s simply no approved tesofensine product sitting on a US pharmacy shelf.
For someone comparing options, this changes the whole shape of the decision. Usually an approved version is the benchmark: a finished, verified product with a label and a regulator’s stamp on it. Tesofensine doesn’t offer that benchmark. So the real choice in the US isn’t “approved versus everything else.” It’s between the two doors that actually exist. If you ever see tesofensine marketed like it’s a proven, approved weight-loss drug, that’s your tell that somebody’s playing loose with the truth.
Worth saying plainly: the approved slot tesofensine doesn’t occupy is exactly where tirzepatide and semaglutide live. Those are FDA-approved, with a mountain of recent evidence behind them. If what you actually want is a proven, approved medication rather than an investigational compound, that’s the honest comparison to make.
Door two: compounded, through a licensed provider watching your numbers
This is the door that exists, and it’s the one that manages the risk I described above, which is why it earns the top spot among the real options.
Here, a licensed compounding pharmacy prepares the tesofensine, and it reaches you with a prescription, after an actual clinician has evaluated you, through a licensed telehealth provider. One useful technical detail: tesofensine is a small molecule, not a peptide, so it wasn’t caught up in the FDA’s peptide-compounding crackdown, and it’s still available through licensed 503A pharmacies with a prescription.
FormBlends operates through exactly this door. It’s a licensed telehealth provider, not a chemical retailer, and pricing tends to run somewhere in the $90 to $300 a month range depending on dose.
Run this door against the three facts from earlier and you’ll see why it separates from door three. The heart-rate cost? A supervised provider takes your baseline heart rate and blood pressure first, decides whether 0.25 or 0.5 mg even makes sense for you, and keeps tracking the numbers. The interaction risk? A clinician checks your current medication list against that serotonergic danger list before anything gets dispensed. The mood question, which the original trials mostly excluded people over? A clinician can actually weigh your psychiatric history, something a spreadsheet never will. Patients who log their dose and symptoms between visits, using something like the FormBlends tracker app, hand their check-ins real data on how their heart rate and side effects have actually moved. That app logs things. It doesn’t sell anything and there’s no checkout involved.
I won’t pretend this door is effortless. It’s slower than clicking “buy now.” There’s an intake, a prescription, and a compounded preparation still isn’t the same thing as an FDA-approved finished drug. But that friction is doing a job. On a compound whose main risk is cardiovascular, and whose interaction list includes some of the most commonly prescribed drugs in America, the screening and the follow-up aren’t red tape. They’re the entire reason this door sits above the next one.
HealthRX (healthrx.com) sits in this same supervised category, for the same reason: real clinical oversight up front, dispensing through legitimate pharmacy channels instead of a chemical-sale website. If you’re choosing between the two, it usually comes down to which one is licensed where you live and which clinical process fits you better.
Door three: the “research chemical” that shows up in a padded envelope
This door exists too, and it manages exactly nothing, which is why it lands at the bottom by a wide margin.
Here, tesofensine gets sold as a laboratory chemical, stamped “for research use only” or “not for human consumption.” That label isn’t just legal boilerplate, it’s the entire reason the product is allowed to exist in that form. The moment somebody markets it for a person to actually take, it becomes an unapproved drug, which is exactly why these sellers put that disclaimer in writing.
Run it against the same three facts and it fails all of them. Nobody takes your baseline heart rate. Nobody is reachable if your resting pulse starts climbing. Nobody checks the vial against whatever’s in your medicine cabinet, so that dangerous overlap with MAOIs, SSRIs, SNRIs, stimulants, and bupropion just sits there, unmanaged. You pick the dose yourself, for a compound whose own developers capped the dose specifically because of cardiovascular concerns. And on top of all that, nothing verifies the powder for identity, strength, or purity. Any certificate of analysis you get is something the seller chose to hand you, not an independent check on anything. Choosing this door means you’re the prescriber, the pharmacist, and the monitoring system, all at once, for a drug whose defining danger is precisely the thing you’re not measuring.
So where does that leave you
Line the three doors up by how much of tesofensine’s known risk each one actually handles, and it isn’t a close call.
The supervised, compounded route sits at the top of the real options, because it’s the only one that does what the evidence actually demands: a cardiovascular baseline, a real look at your medication list, a considered dose, and ongoing follow-up. The research-chemical route sits at the bottom, because it handles none of that and adds the extra worry of a product nobody’s verified. The approved-drug door isn’t even in the running, because for tesofensine, it simply isn’t there yet, and anybody telling you otherwise is misdescribing the compound.
If I had to boil it down for Marcus: tesofensine’s risks are specific and well documented, and they’re precisely the kind of risks that supervision is built to catch. The door with someone watching protects you. The door that just mails you a vial doesn’t. The more you actually understand the heart-rate and interaction story here, the harder that is to argue with.
Straight answers to the questions people actually ask
Can I just get FDA-approved tesofensine somewhere in the US? No. There’s no approved tesofensine product anywhere in the country. It’s classified as investigational, and the furthest along it’s gotten anywhere is that favorable Mexican COFEPRIS committee opinion in early 2023, which again, is not an approval. If a seller talks like it’s approved, they’re not telling you the truth.
Is the compounded version the same drug they used in the trials? Same molecule, yes, prepared by a licensed compounding pharmacy under a prescription. But a compounded preparation isn’t an FDA-approved finished product, full stop. What you’re really paying for in this channel is the oversight around it: the baseline check, the medication review, the monitoring, all of which line up with what the drug’s own risk profile calls for [P1][P5].
If the research-grade stuff is cheaper, why rank it last? Because price isn’t the variable protecting you here. Nothing about the research-chemical channel touches tesofensine’s documented heart-rate or interaction risks, and nobody’s independently verified what’s actually in that vial. Cheap doesn’t mean safe when nobody’s watching the thing that could actually hurt you.
Why does the door matter more for this drug than for some others? Because tesofensine’s signature risks, a documented heart-rate increase and serious interactions with common antidepressants and stimulants, are exactly what supervision is designed to catch and an unsupervised vial simply can’t [P2][P5]. The gap between the supervised route and the research-chemical route is wider here than it would be for a lower-risk compound.
What exactly is tesofensine, and how does it work?
Tesofensine is a triple monoamine reuptake inhibitor, meaning it blocks your brain from reabsorbing dopamine, serotonin, and norepinephrine. It was originally being studied for Parkinson’s and Alzheimer’s disease, and researchers noticed people in those trials were losing weight, which is how it ended up pivoted toward obesity research. It appears to suppress appetite and possibly nudge up resting metabolic rate a bit, but it hasn’t earned FDA or EMA approval for anything as of now.
Does it actually burn fat, or is it mostly appetite suppression?
Honestly, probably some of both, but appetite suppression is the stronger, better-proven part of the story. The Phase 2 data showed real weight loss over 24 weeks, and some researchers think a modest bump in energy expenditure plays a role too. I’d push back on anyone calling it a pure fat-burner, though, because that overstates what the evidence actually shows. Most of the weight loss in these trials looks like it comes from people simply eating less, not from some dramatic shift in how the body handles stored fat.
Is tesofensine a peptide? People keep lumping it in with Ozempic and stuff.
No, and this trips people up constantly. Tesofensine is a small molecule, chemically closer to something like sibutramine than to peptide-based drugs like semaglutide or tirzepatide. That distinction isn’t just trivia either. Peptides usually have to be injected because they break down in the gut, while a small molecule like tesofensine can just be taken as a pill. It also shapes how a compounding pharmacy has to formulate and handle it.
So where does someone actually get this stuff, and what separates the safe routes from the sketchy ones?
Broadly, there are three lanes: unapproved research-chemical sellers, sketchy grey-market supplement sites, and physician-supervised compounding pharmacies. The first two give you zero guarantee on purity, zero accountability on dosing, and zero medical oversight, full stop. The third lane, working through an operation like FormBlends that runs inside proper compounding-pharmacy rules, at least ties the drug to a licensed prescriber and real quality controls. Even that route still carries genuine risk, because tesofensine doesn’t have an approved use yet, so anyone considering it owes themselves an honest conversation with a doctor before doing anything.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm independent of weight loss. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.



